

 A 27-year-old man presents to the emergency department with a 2-day history of hyperemesis followed by episodes of hematemesis. The patient consumed 21 cans of beer 3 days before presenting to ED.
A 27-year-old man presents to the emergency department with a 2-day history of hyperemesis followed by episodes of hematemesis. The patient consumed 21 cans of beer 3 days before presenting to ED.
Background
A 27-year-old man presents to the emergency department with a 2-day history of hyperemesis followed by episodes of hematemesis. He is experiencing worsening epigastric pain, diarrhoea, and myalgia. The patient also describes night sweats and rigors. No melena or hematochezia is reported.
The patient is a binge drinker and consumed approximately 21 cans of beer 3 days ago. The patient’s relevant medical history includes esophagitis, which was diagnosed last year and was treated with a long-term proton pump inhibitor. He has no known drug allergies and has not taken any other medications recently. He does not use any illegal substances.
He has a significant family history of hypertrophic obstructive cardiomyopathy. He works as a labourer and has smoked 10 cigarettes a day for the past 6 years. Soon after presenting in the emergency department, the patient collapses.
Physical Examination and Workup
Upon physical examination, the patient has a temperature of 99.5°F (37.5°C). He is in sinus tachycardia, with a heart rate of 130 beats/min, and his blood pressure is 118/82 mm Hg. The patient is severely dehydrated and agitated, with tenderness to palpation noted in the upper chest and neck. The lungs are clear to auscultation, and heart sounds S1 and S2 are heard, with no murmurs or added sounds. His abdomen is soft, with a tender epigastrium.
The initial work-up includes laboratory investigations. The clinically significant results are as follows:
- White blood cell count: 17.9 × 103 cells/µL (reference range, 4-11 x 103 cells/µL)
- Sodium level: 147 mEq/L (reference range, 135-145 mEq/L)
- Potassium level: 2.6 mEq/L (reference range, 3.5-5 mEq/L)
- Blood urea nitrogen level: 14.5 mg/dL (reference range, 7-19 mg/dL)
- Creatinine level: 1.71 mg/dL (reference range, 0.8-1.7 mg/dL)
Liver function test results are slightly deranged, with the main abnormality being an increased gamma-glutamyltransferase level of 716 U/L (reference range, 11-51 U/L). An ECG is performed and shows a prolonged QT interval, with ST depression in the inferior and anterolateral leads.
The patient is diagnosed with multiorgan failure caused by sepsis, and he is transferred to the high-dependency unit. He is treated with vigorous fluid resuscitation and broad-spectrum intravenous (IV) antibiotics. Further probing of the history reveals that he has vomited 30 times in the past 24 hours.
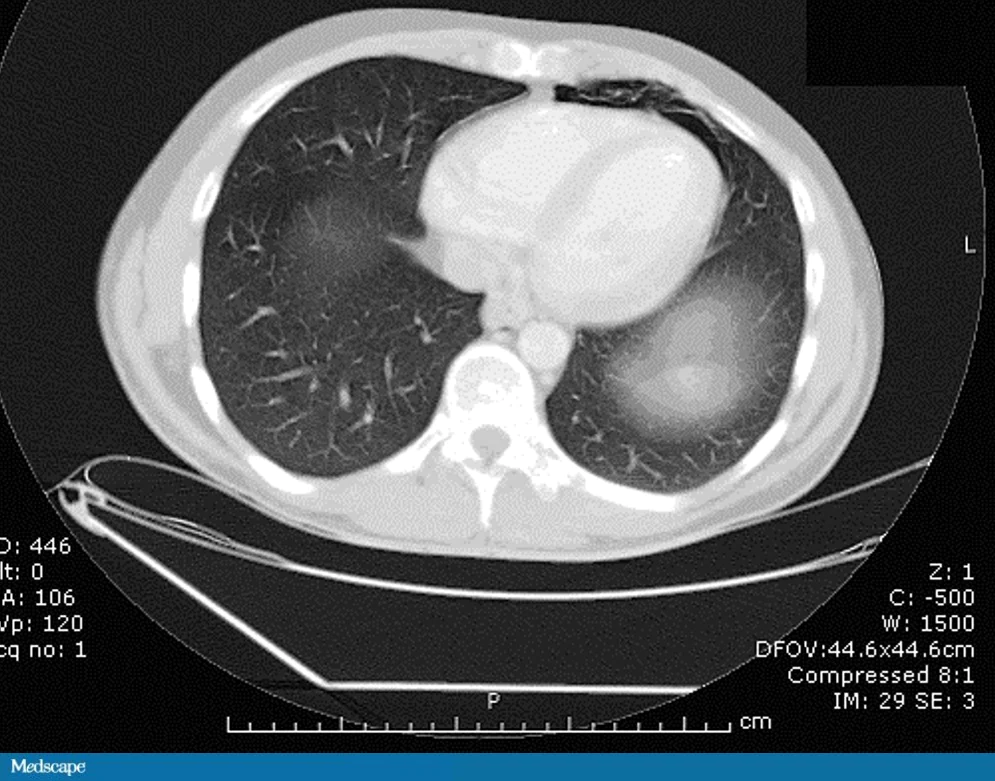
An erect posteroanterior chest radiograph is urgently obtained (Figure 1). An abnormality on the chest radiograph prompts CT of the chest (Figure 2) and the abdomen (not pictured).
Figure 1
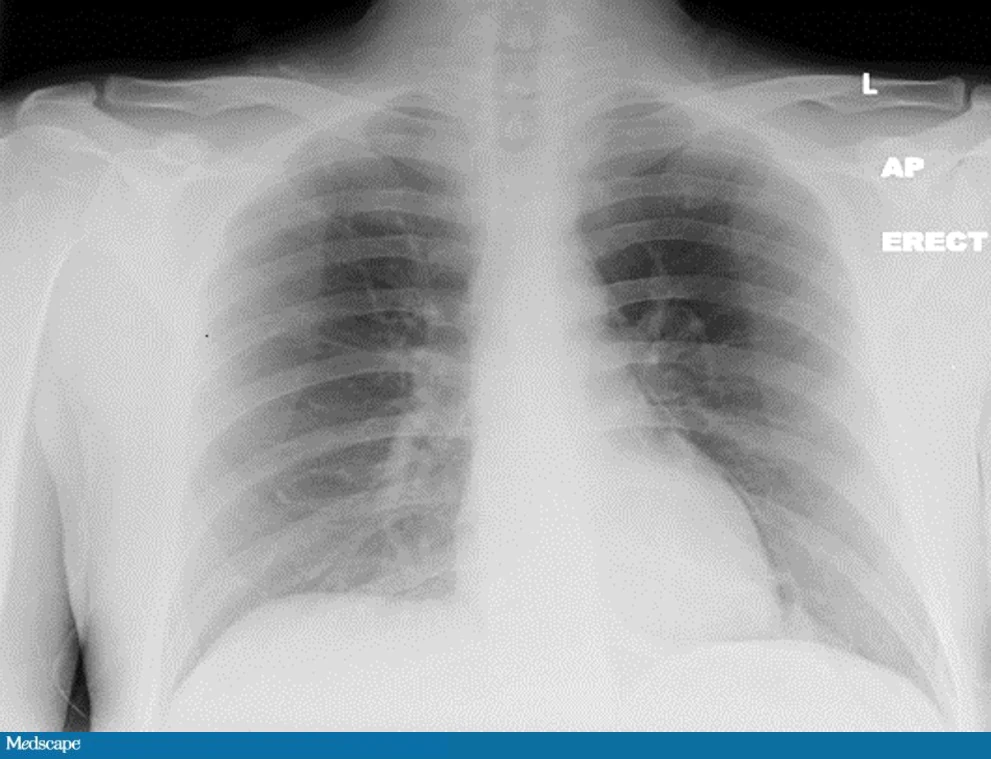
Figure 2
On the basis of only these findings, which is the most likely diagnosis?
- Pneumothorax
- Boerhaave syndrome
- Mallory-Weiss syndrome
- Aortic dissection
Ready to see the answer?
Head to: https://reference.medscape.com/viewarticle/882078_3
More details
- Original story: After Drinking 21 Beers, a 27-Year-Old Can’t Stop Vomiting
- Authors: Gerard J. Fitzmaurice, BSc, MBBCh BAO; Robin Brown, MD, FRCS; Mark E. O’Donnell, DSEM, MFSEM, MRCS; Fionnuala Mone, MBBCh BAO; Angela McGreevy, MBBCh BAO
- All content for this article belongs to Medscape © 2021 WebMD, LLC. For more case examples, visit Medscape Case Challenges.
Do you have a case you are struggling to diagnose? Or a case really unusual case you diagnosed successfully? Share your odd case with Medical Forum at [email protected].