CASE 1
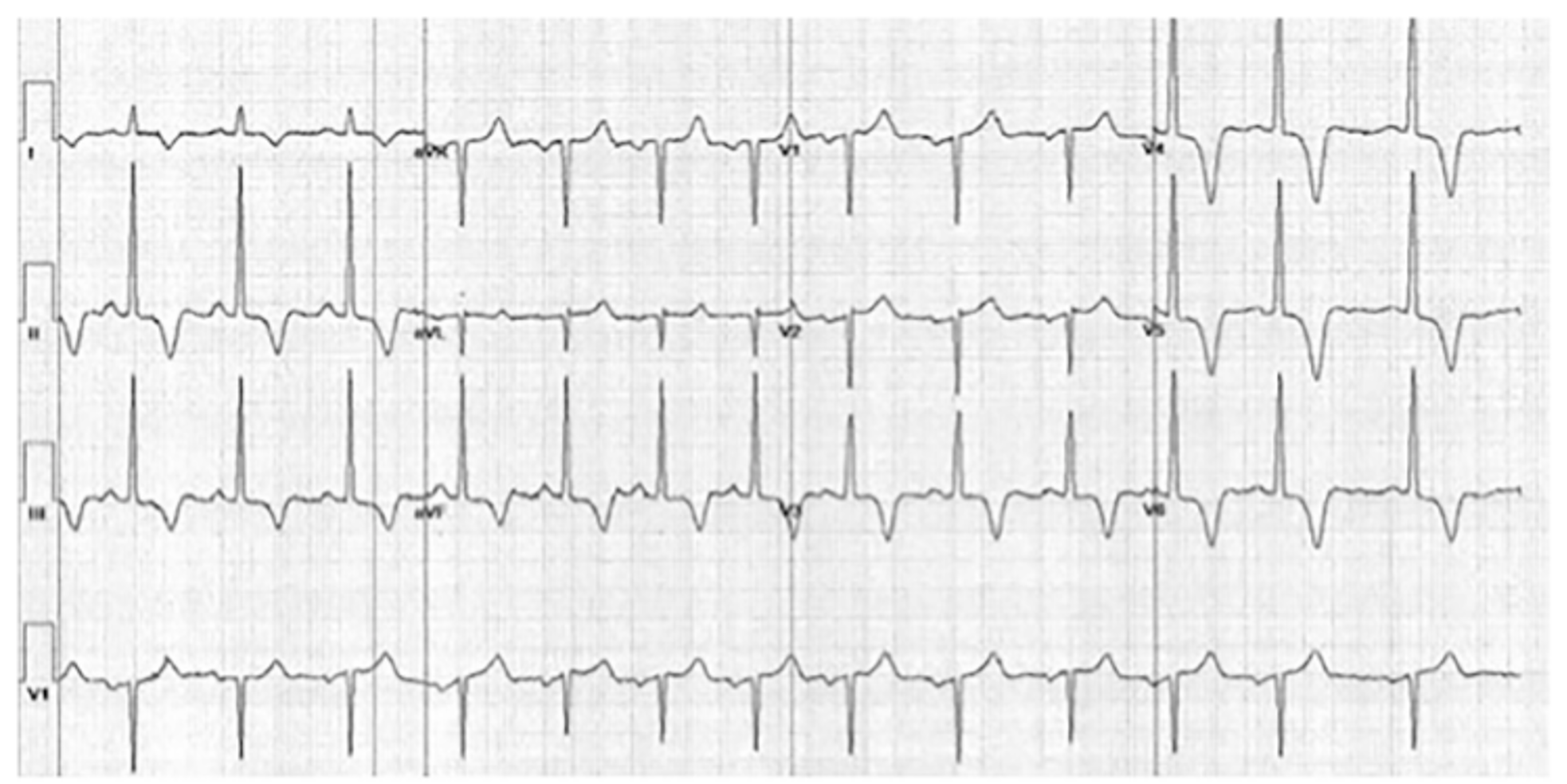
50-year-old male found to have an abnormal resting ECG when he presented to his GP for a “well man check”
- Denied any symptoms of chest pain, syncope, presyncope or palpitations
- No recent illness or new medications
- Background of hypertension on regular Candesartan 8mg
- Fit and active with no reduction in exercise tolerance or heart failure symptoms, scheduled to run a half marathon the following weekend
- No family history of cardiac conditions or sudden cardiac death
- 3 healthy children (15y, 9y, 5y)
- Examination revealed no clinical features of heart failure, 2 heart sounds with no murmur or rub.
#1. The most consistent diagnosis for the following patient with the observed ECG is:
Results
Correct!
Answer: Hypertrophic cardiomyopathy
This ECG shows a sinus rhythm with large voltage QRS complexes (LVH voltage criteria) particularly distributed across the inferior and the more apically placed precordial leads with associated deep T wave inversion. In the context of the clinical picture with no symptoms to suggest ischemia, and no symptoms or examination findings consistent with aortic stenosis, of the available options hypertrophic cardiomyopathy is the most likely diagnosis.
Dynamic T wave inversion in a vascular territory can be seen with coronary ischemia but in this patient the clinical presentation is inconsistent.
Aortic stenosis patients can develop a characteristic ‘strain ECG’ that has a similar appearance to our patient with LVH but usually also has convex, down sloping ST depression and T-wave inversion limited to V5, V6. This ECG can represent LV hypertrophy and myocardial fibrosis [1] which may be prognostic for patients with aortic stenosis and therefore is important to recognise [2].
Our patient’s ECG certainly warrants further evaluation with transthoracic echo imaging. . His echo identified hypertrophy up to 1.8cm (normal <1.0cm) that was most prominent in the apical segmentsThis patient was subsequently diagnosed with apical variant hypertrophic cardiomyopathy (ApHCM).
Hypertrophic cardiomyopathy is predominately a genetically determined disorder of the heart muscle resulting in left ventricular hypertrophy and is usually inherited in an autosomal dominant manner. The ‘classical’ manifestation is with asymmetric septal hypertrophy[3] however various subgroups have been described. Apical variant HCM is where the thickened heart muscle is located at the apex of the left ventricle[4].
Apical variant HCM accounts for 10-25% of hypertrophic cardiomyopathy cases[3] and it is much more common in Asian men, it has also been known as Yamaguchi syndrome[5]. This variant has fewer patients reporting a family history, it does not cause left ventricular outflow tract obstruction (LVOTO) or mitral regurgitation and whilst it was initially thought to be a benign variant, data suggests an annual cardiac death rate of 0.5-4%[3, 4].
This patient’s children should undergo screening ECG and transthoracic echo imaging at the time of his diagnosis then every 3-5 years[6].
In regard to the patient’s recreational physical activity and participation in the upcoming half-marathon, it would be recommended that he undergo specialist evaluation and shared decision making about participation in vigorous exercise. There is data that supports safe participation in vigorous exercise in asymptomatic HCM patients[6].
Wrong answer! Please refresh page and try again