

 A 70-year-old man presents with a history of initial fullness in the left medial epitrochlear region that developed over approximately 2 months into a golf ball–sized mass.
A 70-year-old man presents with a history of initial fullness in the left medial epitrochlear region that developed over approximately 2 months into a golf ball–sized mass.
Challenge
A 70-year-old man presents with a history of initial fullness in the left medial epitrochlear region that developed over approximately 2 months into a golf ball–sized mass. The mass is nontender, with no drainage. The overlying skin is normal, and the patient does not recall any trauma. He describes no other symptoms and denies fever, sweats, or weight loss, as well as any loss of muscular function or tingling, burning, or pain sensations of the left arm. The mass causes mild to no discomfort, and the patient is mainly concerned about its rapid progression.
He has a past medical history of familial hypercholesterolemia and gastroesophageal reflux disease (GERD) with esophagitis, which are managed with atorvastatin and omeprazole, respectively. He has never smoked tobacco or used alcohol or illicit substances. His surgical history includes a hernia repair and a tonsillectomy. He has a family history of heart disease and Alzheimer’s disease.
Physical Examination and Workup
The patient is oriented to person, place, and time but is in acute distress in regard to the rapid development of the mass. His height is 5 ft 10 in (177.8 cm), and his weight is 216 lb (97.98 kg), with a body mass index of 31 kg/m2. His oral temperature is 98.7°F (37°C). His pulse is 80 beats/min and regular, his respiration rate is 16 breaths/min and unlabored, and his blood pressure is 112/70 mm Hg in the left upper extremity when he is seated. His oxygen saturation measured by pulse oximetry is 97% on room air.
Heart sounds are normal, and the rate and rhythm are regular. The lung examination reveals no dullness or hyperresonance to percussion, and breath sounds are normal across all lung fields. The abdomen is nontender, with no guarding or organomegaly, and bowel sounds are normal. A firm 4 cm × 3 cm mass is noted in the epitrochlear region of the left elbow. The extremities exhibit normal tone and motor strength, with no contractures, malalignment, tenderness, or bony abnormalities. No cyanosis, edema, or varicosities are noted in any of the extremities. Inspection and palpation of the skin reveal no abnormalities.
A CT scan with contrast shows a 4.0 cm × 3.1 cm soft tissue density in the medial, supracondylar region of the left arm, slightly above the elbow. The mass does not exhibit significant enhancement. It exerts a mass effect on the adjacent basilic vein with extrinsic compression. The fat planes between the mass and the underlying musculature appear preserved, with no infiltration, but some induration in the adjacent fat is noted. The surrounding soft tissue and bones appear normal. The CT scan results are highly suggestive of a soft tissue mass that probably requires pathologic examination. See the images below.
Figure 1
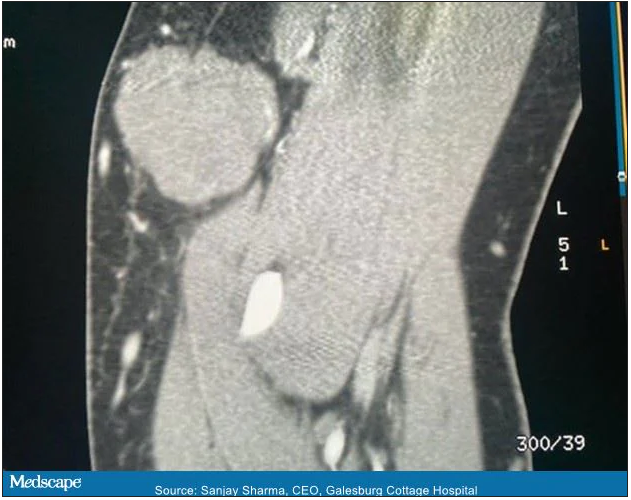
Figure 2

The mass is excised. The surgical pathology specimen consists of a 1.9 cm × 1.4 cm × 0.3 cm oval portion of homogeneous, glistening yellow-tan adipose tissue and a 4.4 cm × 3.7 cm × 3.2 cm oval portion of soft, gelatinous pink-grey tissue. The adipose tissue in the specimen is part of the overlying skin that was removed for appropriate closure of the incision.
On the basis of these findings only, what is the most probable diagnosis?
- Lipoma
- Rheumatoid nodule
- Infectious mononucleosis
- Diffuse large B-cell lymphoma
Ready to see the answer?
Head to: https://reference.medscape.com/viewarticle/962080_2
More details
- Original story: What’s Causing This Rapidly Growing, Golf Ball–Sized Mass?
- Author: Mark Davis, MD; Nandita Kakar
- All content for this article belongs to Medscape © 2021 WebMD, LLC. For more case examples, visit Medscape Case Challenges.