

 New updates to the Australian Asthma Handbook encourage doctors to change the way they prescribe for and treat the respiratory condition.
New updates to the Australian Asthma Handbook encourage doctors to change the way they prescribe for and treat the respiratory condition.
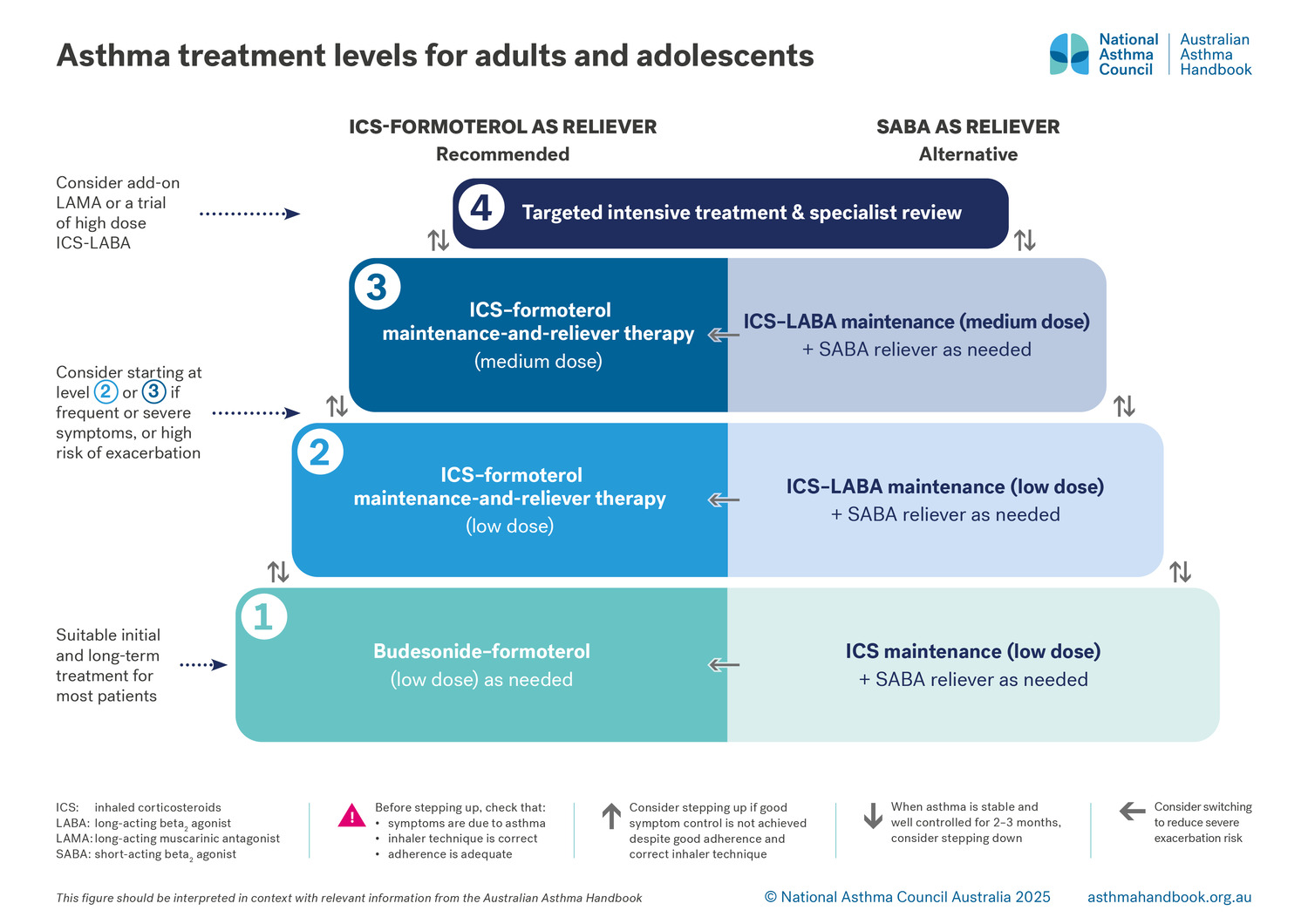
The updates advise doctors to stop prescribing or advising treatment with as-needed short-acting beta2 agonists (SABA) alone to manage asthma in adults and adolescents.
Put together by the National Asthma Council Australia (NAC) the guidance now recommends anti-inflammatory reliever (AIR) only therapy and maintenance-and-reliever therapy (MART) for adults and adolescents aged over 12.
Dr Brett Montgomery, Perth GP and member of the NAC Guidelines Committee told Medical Forum inhaled corticosteroids (ICS) were now indicated for all adults and adolescents with asthma.
“The last lot of guidelines said that there was a small number of people we could manage on short-acting beta agonists alone – people who had not had an exacerbation in the last year and only got their symptoms rarely. Many international guidelines have moved away from allowing that and we have followed suit in this new addition,” he said.
RELATED: Navigating therapy for severe asthma made simpler with new resources
“Now, if you’re an adult or an adolescent who has asthma, we don’t think anyone should be managed on short beta agonists alone, instead we think everyone should have treatment that includes an inhaled corticosteroid. Our preferred starting approach will be to use a combination inhaler containing budesonide-formoterol.”
In terms of diagnosis, doctors should consider the use of fractional exhaled nitric oxide (FENO) testing in addition to spirometry as another way of proving a diagnosis.
“Nitric oxide is a chemical that is produced in our body when there’s inflammation going on. It’s important in blood vessels but can also be detected in tiny amounts in expired breath. If it’s above a certain threshold then we say that is also evidence of asthma” he said.
Dr Montgomery said this testing gave doctors another way of proving a diagnosis for some people, as the intermittent nature of asthma could mean the condition did not show up in spirometry testing because the patient may not be experiencing symptoms at the time.
RELATED: Predicting childhood asthma before onset
He said the use of short-acting beta agonists alone for children was still an option.
“There is still, we feel, an appropriate place for some young children to be treated with short-acting beta agonists alone if they have mild infrequent symptoms and they haven’t had a severe exacerbation and ended up in hospital in the last year or so.”
Dr Montgomery added that the thresholds for the use of inhaled corticosteroid in children had changed slightly.
“We have a clear chart that gives me a clear recommendation of whether this child does or does not merit the use of corticosteroid, which helps to back up clinical judgement.”
For those few patients with severe asthma that were not responding to treatment, doctors are encouraged to look at addressing why.
“I always think ‘are they taking the treatment’ or ‘have they got good inhaler techniques’ so that they know how to take and use their puffer well,” Dr Montgomery added.
The new guidelines emphasised the importance of referral to appropriate specialists instead of increasing prescriptions or dosages.
“If asthma symptoms are still uncontrolled despite escalating therapy, we are wanting to emphasise the importance of referral to respiratory specialists to consider what’s called monoclonal antibody treatment,” Dr Montgomery said.
Want more news, clinicals, features and guest columns delivered straight to you? Subscribe for free to WA’s only independent magazine for medical practitioners.
Want to submit an article? Email [email protected]