

The COVID state of emergency ended with health worker vaccine mandates quietly revoked in November. The mandates were imposed to “limit the spread of COVID-19 among vulnerable populations in Western Australia” and to “abate the risk to health care workers and health support workers who are at a higher risk of exposure”, the Chief Health Officer said. It is difficult to find any robust evidence supporting this policy.

There was never convincing evidence the vaccines limit the spread. That they were needed to protect the vulnerable was based more on hope, good intentions and hypothetical modelling than critical appraisal of real-world evidence.
mRNA injections stimulate circulating antibodies that reduce disease severity once the virus reaches the alveoli, but do not confer mucosal immunity. This was corroborated by early studies that showed similar nasal viral loads in the vaccinated and unvaccinated. Even before mandates were introduced, breakthrough infections were commonly observed.
The randomised controlled trial securing emergency authorisation did not consider transmissibility as an outcome (confirmed in the European Parliament by a Pfizer executive).
Since Omicron, new subvariants have spread at a high rate despite 95% of our population double vaccinated and over 80% triple vaccinated. With each successive dose, we’ve seen vaccine effectiveness become weaker, shorter lasting and eventually negative. New South Wales health surveillance data consistently show a direct correlation between number of vaccinations and population rates of hospitalisation.
This makes immunological sense as the injections were designed to produce antibodies to the Wuhan spike protein, but with over 30 mutations there has been inevitable immune escape. The antibody response to the original antigen led to immune imprinting, a phenomenon that impairs the immune system’s ability to respond to later variant antigens, explaining empirical evidence that vaccinated people remain infective longer than unvaccinated.
The vaccines failed to limit COVID spread. Mass vaccination campaigns and mandates may have prolonged the pandemic. Our World in Data shows much lower COVID case numbers in countries with low vaccination rates, both across the board and in specific regions when we compare high income with upper middle and lower middle-income countries (e.g. Australia vs South Africa, or Israel vs Jordan).
The vaccine’s inability to prevent infection or transmission was acknowledged by the US CDC in August, when it stopped differentiating its public health guidance between the vaccinated and unvaccinated.
 “Do it for others” has ultimately proven to be little more than a collectivist myth based on non-existent or, at best, flimsy data.
“Do it for others” has ultimately proven to be little more than a collectivist myth based on non-existent or, at best, flimsy data.
As the mRNA injections do not prevent transmission, but may reduce disease severity, they can be considered preventative treatment rather than true vaccines. Thus, people should have the right to freely choose treatment based on their personal weighing of benefits and risks.
Mandating treatment rejects core ethical principles of informed consent and bodily autonomy. The Australian Immunisation Handbook emphasises that, before vaccination, valid consent must be given voluntarily “in the absence of undue pressure, coercion or manipulation”.
Using novel technology that was rushed to market, these injections remain experimental while effectiveness and safety data are collected and evaluated. Mandating experimental treatment runs counter to the Hippocratic Oath and Nuremberg Code.
In working age people where mandates applied, COVID is overwhelmingly a mild disease. Australian data show a case fatality rate below 0.1% in the 20-70-year age group. It remains unclear why well-researched pandemic preparedness plans updated less than a year before the outbreak were binned, while a risk-stratified approach was ignored as advocated in the Great Barrington Declaration.
This would have seen “focused protection” measures including vaccination targeting the old and vulnerable while allowing others to make their own risk-informed decision.
The vaccines were promoted as “95% effective” based on the relative risk reduction of symptomatic infection, rather than the absolute risk reduction of only 0.84%. At 0.1% case fatality rate, the absolute risk reduction for COVID death is thus 0.00084%, or a 1 in 119,000 chance that the vaccine prevents death in this age group.
To balance this with the potential harms, we need to consider that the mRNA injection instructs our cells to manufacture the toxic spike protein, which damages endothelial cells and is highly inflammatory and thrombogenic.
After vaccination, spike protein is biodistributed widely and persists longer at higher plasma levels than after infection. Whereas natural mRNA breaks down within hours, synthetic mRNA and spike protein are still detected in lymph nodes two months after the second dose.
Pharmacovigilance data show an unprecedented number of serious adverse events, mostly in those under 70. Clinical trial data showed a 1 in 800 absolute risk of serious adverse events after vaccination, far exceeding the risk of COVID hospitalisation (cardiac injury most reported). Two studies detected subclinical myocarditis in 2.8% of young men based on post-vaccination troponin levels.
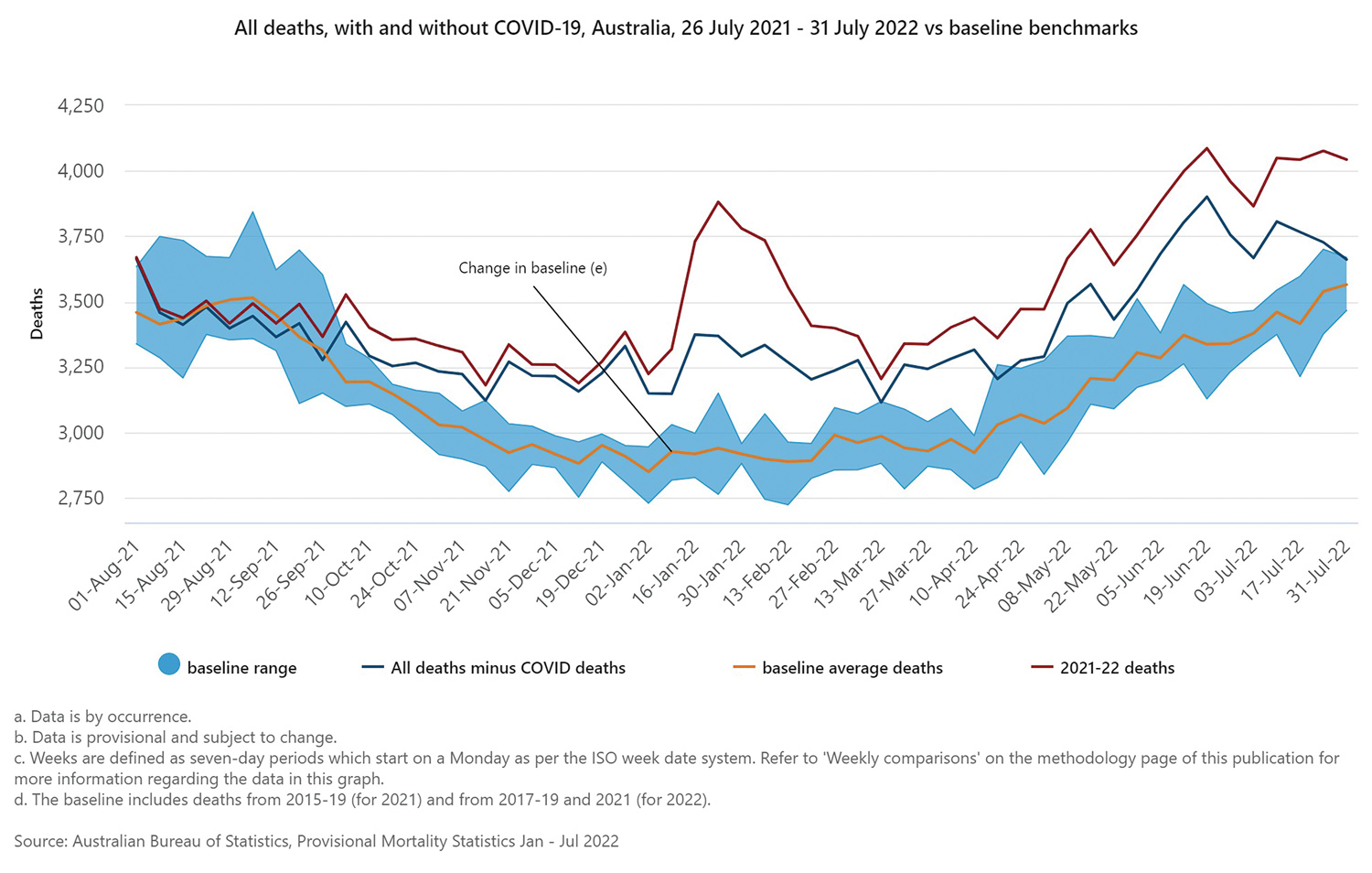
We are currently witnessing excess mortality across the Western world (Australia 17% above the five-year baseline). The excess mortality curve started its rise at the height of the vaccination campaign before our borders opened and infections peaked (see ABS graph). Most of the excess deaths are non-COVID related. Actuarial and life insurance data overseas show the excess mortality occurring mostly in the young and employed population.
The exact cause of excess non-COVID deaths is yet to be characterised but may be collateral damage from our pandemic response. They cannot be automatically linked to the vaccines, yet a causal relationship cannot be ruled out. Almost two years into the roll-out, it is disturbing that no government or health authority promoting the vaccines has seriously looked at analysing these concerning safety signals.
In an age group at minimal risk from the disease, even if at higher risk of exposure in the health-care setting, it is perplexing why health worker vaccine and booster mandates applied for so long while evidence of net vaccine harm was available.
We need more open, honest and robust debate and an independent inquiry into the government’s COVID vaccine policy and wider pandemic response. We must learn lessons and there must be accountability so that future mistakes can be avoided.
References
1. Household transmission of the SARS-CoV-2 Omicron variant in Denmark – PMC (nih.gov).
2. Duration of Shedding of Culturable Virus in SARS-CoV-2 Omicron (BA.1) Infection | NEJM
3. Fifty Years Later: The Significance of the Nuremberg Code | NEJM
4. Curing the pandemic of misinformation on COVID-19 mRNA vaccines through real evidence-based medicine – Part 1 | Malhotra | Journal of Insulin Resistance
5. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults – ScienceDirect
6. Cardiovascular Effects of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents[v1] | Preprints
7. Mueller, Christopher. Myocardial Injury after mRNA booster vaccination. Presented at European Society of Cardiology conference 28 August 2022 EUROPEAN-SOCIETY-CARDIOLOGY-CONGRESS-AUG22-MUELLER-MYOCARDIAL-INJURY-AFTER-mRNA-BOOSTER.pdf | DocDroid
– More references on request
ED: As noted this article is the opinion of the author.