

 A new national standard on emergency laparotomy care is set to be introduced.
A new national standard on emergency laparotomy care is set to be introduced.
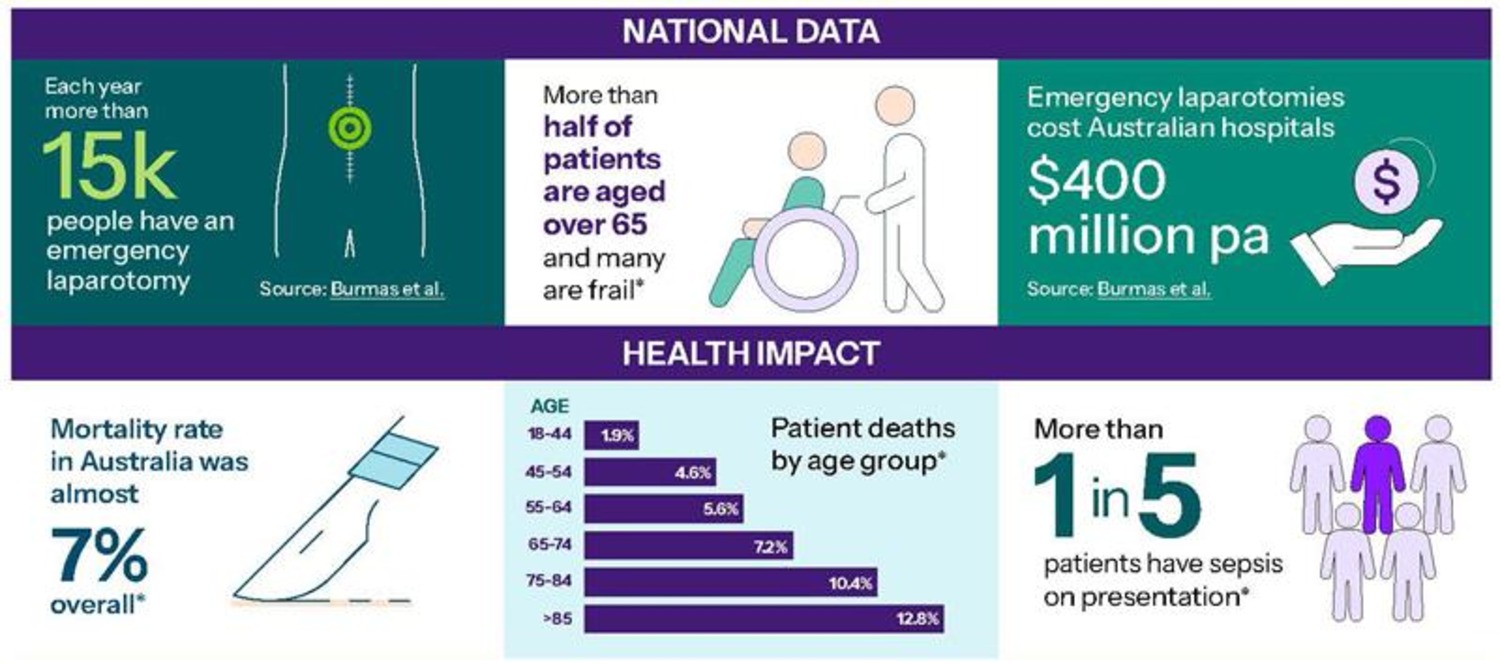
Focusing on emergency laparotomy for urgent conditions affecting the gastrointestinal tract, like a bowel obstruction, perforation or serious internal bleeding, it is expected to improve care for more than 15,000 Australians each year.
The Australian Commission on Safety and Quality in Health Care will launch the first Emergency Laparotomy Clinical Care Standard at the Royal Australasian College of Surgeons Annual Scientific Congress in Perth on May 1.
Unlike other life-threatening medical emergencies such as stroke or cardiac events, evidence-based clinical pathways for urgent abdominal conditions are not consistently embedded in practice.
This is despite emergency laparotomy being one of the highest-risk surgical procedures, with recovery taking weeks or months, and patient outcomes varying significantly.
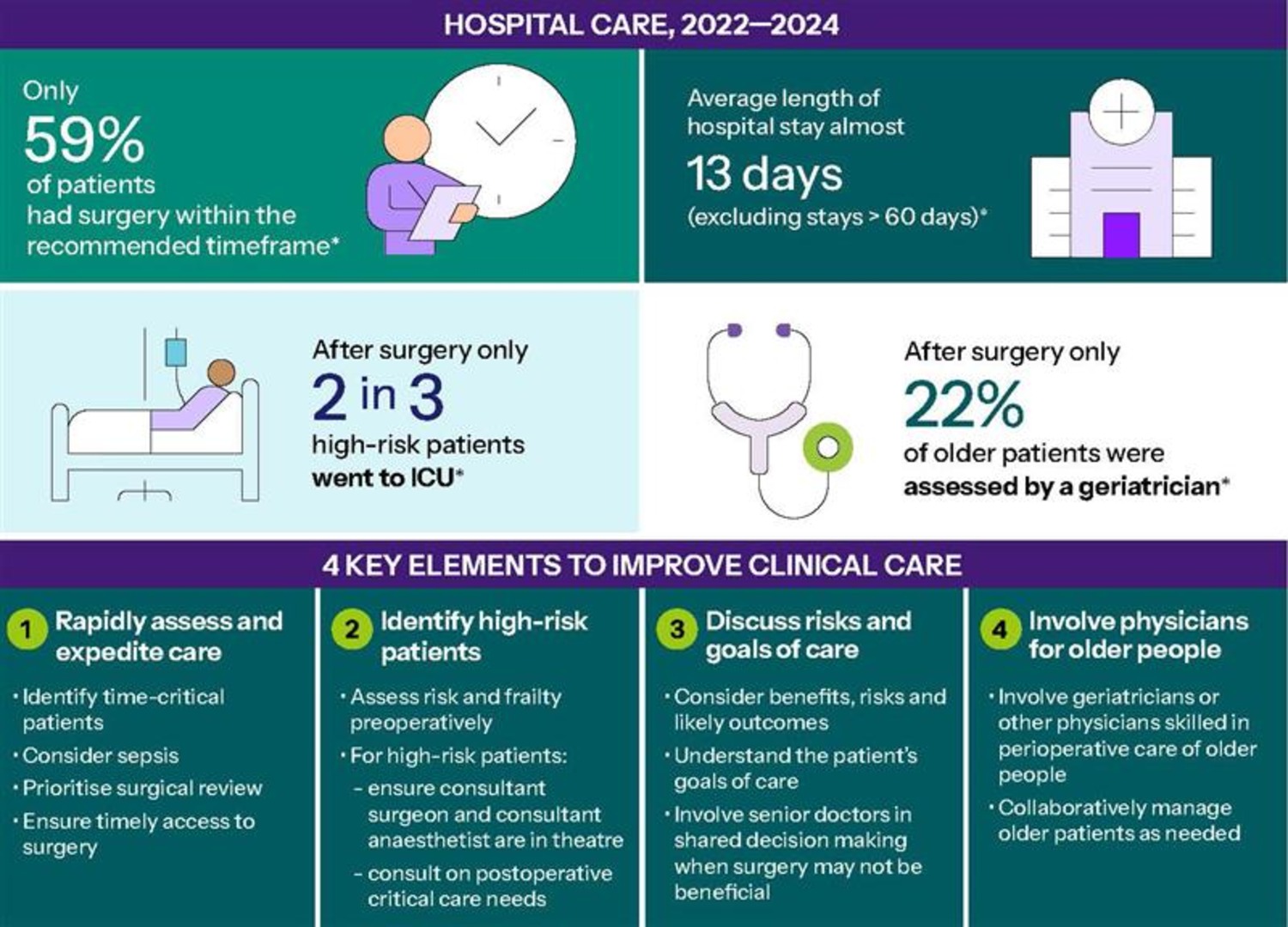
According to the Commission, the mortality rate for people undergoing the procedure in Australia is almost 7% overall and it is substantially higher for people who have sepsis or who are older or frail.
RELATED: New clinical guidelines for bowel cancer are on the way
The key elements of the standard focus on rapidly assessing and expediting care, identifying high-risk patients, discussing risks and goals of care and involving physicians for older patients.
Commission Medical Advisor Dr Phoebe Holdenson Kimura said the Standard was a call to action for health services to consider the entire patient journey, from when a critically ill patient presented and was assessed in the emergency department, through to surgery, postoperative care and discharge.
“Timeliness is crucial, and so is understanding the patient’s level of risk,” she said.

“The use of risk scores can create a common language and support decision-making to help ensure patients receive appropriate care.
“For high-risk patients, this includes having a consultant surgeon and consultant anaesthetist for their surgery and will often mean admission to ICU after their operation,” she said.
Professor David Watters, a surgeon with Deakin University, said an hour or two could make a big difference to the chances, or degree, of recovery after emergency laparotomy.
“I’ve seen first-hand how patients can suffer because of late presentation, delayed diagnosis or referral, late recognition of complications, or failure to manage their other medical conditions,” he said.
Dr Watters said the standard provided an opportunity to reduce variation between health services by ensuring consistency in how to provide the best care to patients at the right time and in the right place.
The standard reminds practitioners to consider benefits, risks and likely outcomes of emergency laparotomy care.
Dr Holdenson Kimura said for some high-risk emergency laparotomy patients, the risks of surgery would outweigh the benefits.
“The care team must quickly assess the situation and involve the patient and their family in treatment decisions, especially when surgery may not be beneficial,” she said.
“These discussions can be difficult, but it is so important that skilled clinicians help these patients and their families to understand the risks, including the likely impacts on their quality of life.”
The Standard was developed in collaboration with key stakeholders including the Clinical Quality Registry, the Australian and New Zealand Emergency Laparotomy Audit – Quality Improvement (ANZELA-QI), which is updating their data collection and key indicators in line with the Standard.
Want more news, clinicals, features and guest columns delivered straight to you? Subscribe for free to WA’s only independent magazine for medical practitioners.
Want to submit an article? Email [email protected]