

 The Kimberley region is experiencing a diphtheria outbreak with 42 cases recorded in the region so far this year.
The Kimberley region is experiencing a diphtheria outbreak with 42 cases recorded in the region so far this year.
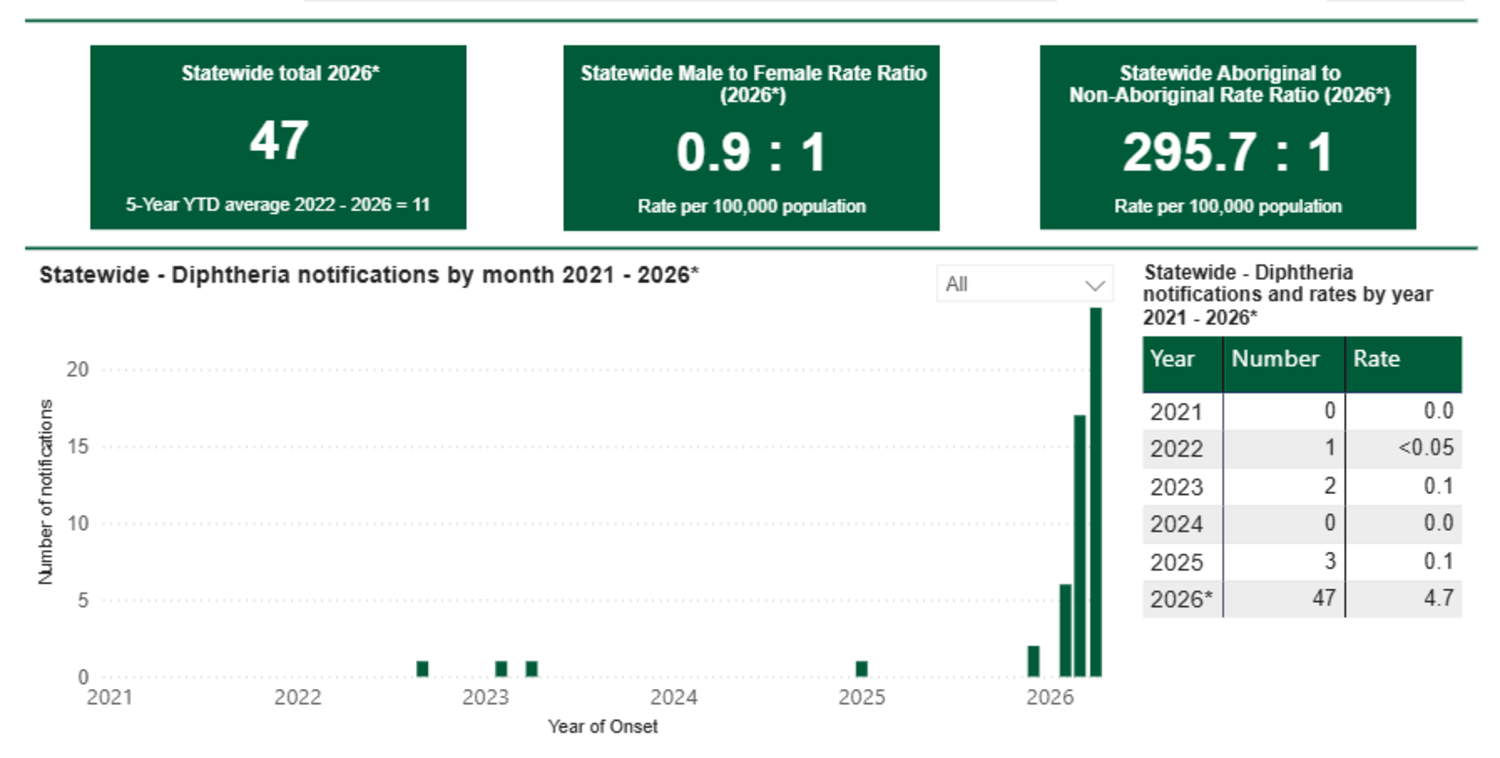
There have been 47 cases across Western Australia in the past four months, almost eight times the total amount of cases recorded throughout the previous five years.
There have been two cases recorded in both the Pilbara the Goldfields, and one in the Perth Metropolitan area so far this year.
Some of the cases have been of the extremely rare respiratory diphtheria, which had not been recorded in WA for more than 50 years.
WA Health’s Director of Communicable Disease Control Dr Paul Armstrong issued a clinicians alert in March about the outbreak.
In it he warned doctors to be vigilant for patients in or from the Kimberley, and potentially the Pilbara or Goldfields regions, presenting with clinically suspicious skin sores, infected wounds, or upper respiratory illness.
The alert reminded doctors they need to urgently notify suspected or confirmed diphtheria cases to their local Public Health Unit by phone and not to wait for laboratory confirmation before notifying.
Cutaneous and respiratory diphtheria are vaccine-preventable diseases caused by toxigenic strains of Corynebacterium diphtheriae (and occasionally C. ulcerans).
RELATED: No easy cure – the drive behind vaccine hesitancy
The bacteria produce an exotoxin that causes damage to the mucous membranes of the respiratory tract or skin and may lead to complications such as myocarditis and neuropathy.
Dr Armstrong noted in the alert that diphtheria is rare in Australia due to high vaccination rates and improved living conditions, but increasing cutaneous disease among Aboriginal people had been reported in Queensland and the Northern Territory.
Most of the cases in WA this year have been in Aboriginal people. While cases have been recorded within the 0-4 years age group all the way up to people in the 70s, 15 cases have been in those in their 20s.
Cutaneous diphtheria usually presents on exposed limbs as secondary infection of skin lesions or wounds, or as primary punched-out ulcers with well demarcated edges and a grey necrotic slough.
Cutaneous disease is rarely associated with systemic toxicity but plays an important role in transmission through contact with wounds or contaminated fomites and can cause respiratory disease in contacts.
Respiratory diphtheria typically presents with initial fever and sore throat, with patches of discoloured pharyngeal exudate that may thicken to form an obstructive and life-threatening pseudomembrane.
Swabs should be taken from any lesions and another combined swab of nasopharynx and throat, specifying culture for diphtheria on the pathology form before starting antibiotics.
Want more news, clinicals, features and guest columns delivered straight to you? Subscribe for free to WA’s only independent magazine for medical practitioners.
Want to submit an article? Email [email protected]